
By Amanda Dawson, B.Sc., M.Sc. P
The pelvic floor is an area of the body that was most likely left out of your grade 7 health class, but it participates in everything we do, every day.
We can find this group of supporting muscles, ligaments and tendons at the base of our abdominal canister. It helps to create stability with motion (lifting anything), draws blood flow into and out of the lower part of body, has sexual function, and contracts to allow us to hold stuff in, then releases to let go of anything we want out (think bowel and bladder functions). Anatomically speaking, male and female pelvic floors are surprisingly similar.
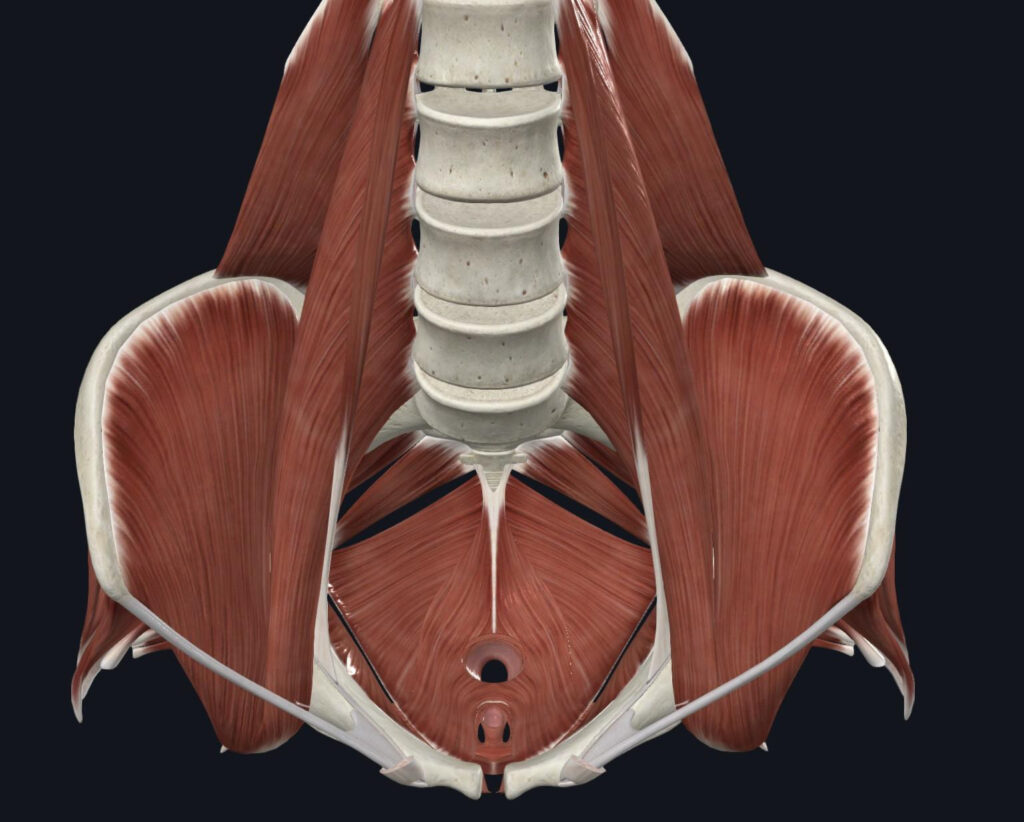
We are increasingly understanding the importance of looking at pelvic floor function in relationship to the rest of the components of the aforementioned abdominal canister. If we consider the pelvic muscles in the photo above as the floor, then we may consider the ceiling to
be our diaphragm. The walls would be our abdominals and low back muscles.
Commonly, we hear about pelvic floor strength. It has been decided colloquially that stronger is better. We as clinicians hear many stories of people being told to just “do more Kegels” to aide their pelvic organ prolapse, urinary incontinence, and essentially any other
pelvic floor dysfunction. The problem is – Kegels (aka pelvic floor contractions) alone do not teach us how to move the canister all together.
Let me introduce you to the concept of intra-abdominal pressure (IAP). When we look at the canister created by our pelvic floor, diaphragm, abdominals and low back, we might be able to picture it like a piston in an engine. As the diaphragm descends to fill our lungs, the pelvic floor moves in the same direction at the same time. The system coordinates. When we laugh, cough or sneeze, the system creates enough pressure to expel air out. Try a little cough with your hands around your lower rib cage to feel what I mean. When we lift something heavy, that stable feeling in our midsection comes from the system contracting and closing all exit points to create more IAP. The pressure creates force and control. Each component of the system has to manage this pressure properly and in perfect timing, otherwise we can picture this piston more like a tube of toothpaste with the cap off.
Mismanagement of the IAP appears to be correlated with many common dysfunctions (incontinence, back pain, internal pain, etc.) and is especially visible in higher intensity sports such as running, power lifting, and CrossFit where the pressures are more exaggerated. It’s important to be assessed by a professional who can tell you how all your parts work together – and which area of your system to focus on. The good news is, IAP mismanagement is often something that can be fixed with a little concentration and the right rehabilitation process, and most of the time your therapist will help you find ways to continue doing whatever it is that floats your IAP boat.
We now know how important this system is for your daily movement, make sure you read the owners manual and do all the proper maintenance!
Raizada V, Mittal RK. Pelvic floor anatomy and applied physiology. Gastroenterol Clin North Am. 2008 Sep;37(3):493-509, vii. doi: 10.1016/j.gtc.2008.06.003. PMID: 18793993; PMCID: PMC2617789.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2617789/
Park H, Han D. The effect of the correlation between the contraction of the pelvic floor muscles and diaphragmatic motion during breathing. J Phys Ther Sci. 2015 Jul;27(7):2113-5. doi: 10.1589/jpts.27.2113. Epub 2015 Jul 22. PMID: 26311935; PMCID: PMC4540829.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4540829/
